The Journey Begins
Welcome to our blogsite. We wish you have a healthy pregnancy and a happy journey to motherhood. This milestone is one of the significant moments in one’s life and we hope you’ll have a pleasant experience during this time. Browse through our page and discover that a painless labor is possible!

Good company in a journey makes the way seem shorter. — Izaak Walton
Identifying the Patient in Labor
| Characteristics | True labor | False labor |
| Contractions:
Frequency Interval Intensity |
Regular Shortens Increases |
Irregular Remains long Remains unchanged |
| Cervix | Dilates | Does not dilate |
| Discomfort | Back and abdomen | Lower abdomen |
| Sedation | Discomfort not relieved by sedation | Discomfort relieved by sedation |
Examination of the Patient
The diagram below shows how the cervix is assessed or you may watch a video on how to do a pelvic exam operationalmedicine.org/ed2/Video/pelvic_exam_video.htm

Cardinal Movements of Labor
| Engagement | The biparietal diameter—the greatest transverse diameter in an occiput presentation—passes through the pelvic inlet
|
 |
| Descent | First requisite
Brought about by one or more of four forces: (1) pressure of the amnionic fluid (2) direct pressure of the fundus upon the breech with contractions (3) bearing- down efforts of maternal abdominal muscles, and (4) extension and straightening of the fetal body. |
 |
| Flexion | Produced by the resistance of the fetal head whether from the cervix, walls of the pelvis, or pelvic floor
Conversion from OF to SOB
|
 |
| Internal Rotation | essential for the completion of labor, except when the fetus is unusually small.
|
 |
| Extension | Produced by forces exerted by the uterus, acts more posteriorly, and the second, supplied by the resistant pelvic floor and the symphysis, acts more anteriorly bringing the base of the occiput into di- rect contact with the inferior margin of the symphysis pubis
|
 |
| External Rotation | Brings the presenting part to its original position
|
 |
| Expulsion | the anterior shoulder appears under the symphysis pubis, and the perineum soon becomes distended by the posterior shoulder.
|

|

What is Epidural Analgesia?
Epidural analgesia is an injection of local anaesthetic alone, or more commonly in combination with pain. The injection is usually made in the lumber region at the L2/3 or L3/4 space.

What is Epidural Analgesia Used for?
Epidural labor analgesia may be performed to relieve the pain of labor and to provide an in-situ epidural catheter for rapid conversion to surgical anesthesia for operative delivery, should it become necessary.
Pain relief — Epidural analgesia is appropriate for laboring women regardless of parity, cervical dilation, and fetal station, unless there is a contraindication. Maternal request is sufficient indication for pain relief during labor, barring a medical contraindication. It is also indicated for several obstetric situations such as:
- Prolonged labour
- Difficult forceps delivery
- Maternal exhaustion during labor
- Pre-eclampsia
- Unacceptable pain during labor
The technique is usually easily performed, life-threatening complications are rare, and side effects such as pruritus and hypotension are transient or easily treated.
How Does Epidural Analgesia Work?
Epidural analgesia provides complete motor (causing paralysis) and sensory blockade (causing loss of sensation), around or near the site of pain while allowing the patient to remain conscious. The level of epidural block usually extends distal from the upper abdomen. As a consequence of epidural analgesia; women become immobile and require more frequent observations from the medical staff.
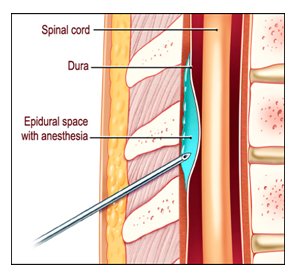
Medication is delivered through a catheter – a very thin, flexible, hollow tube – that’s inserted into the epidural space just outside the membrane that surrounds your spinal cord and spinal fluid. An epidural is the most commonly used method of pain relief for labor in the United States.
What is the procedure like?
You lie curled on your side or sit on the edge of the bed while an anesthesiologist cleans the injection site, numbs the area, then carefully guides a needle into your lower back.

The anesthesiologist then passes a catheter through the needle, withdraws the needle, and tapes the catheter in place. At this point, you can lie down without disturbing the catheter, and medication can be administered through it as needed.
Important Issues Regarding Epidural Analgesia
Before the anesthesiologist administer epidural analgesia you must provide consent and tell your doctor if you have:
- history of hypersensitivity or allergy to any previous medications including anesthetics and opioids
- local inflammation or infection
- spinal deformity or previous spinal surgery
- bleeding or clotting disorders
- cardiovascular disease/s such as heart failure, cardiac ischemia, hypertension or hypotension and/or any other cardiac complications
- nervous system disease
- neuromuscular disease such as myasthenia gravis
- any other medical conditions
If you are taking any medication/s, you must inform your doctor prior to the procedure.
